




I spoke with specialist occupational therapist Rosie Dear, about the work they are doing within oncology. Rosie and the University Hospitals Leicester team have started working with breast cancer patients in the last couple of years, alongside their main work in hands, burns and trauma.
The service was started as Rosie had been made aware of an OT in the USA using the BTE PrimusRS with breast cancer patients and getting really good results. Rosie made contact with the breast care team and they agreed to run a pilot and this case study was one of the first people that came through.
Patient case study: Ms A
41-year-old teacher who before she got Breast Cancer was fit and well with no medical history of note.
- She had a left sided mastectomy.
- She had initial surgery 6 months before she was referred. Following surgery she had more surgery to remove more lymph nodes a couple of months later followed by radiotherapy and chemotherapy.
- After chemotherapy, she developed cording and mild lymphoedema so was being treated by specialist lymphoedema team.
- Her main worry was the pain level and discomfort. There was very painful and restrictive scarring in pec area especially in abduction and this meant reduced movements. She wouldn’t put hand over her head which wasn’t helping as the tissue needed to be lengthened.
- She had reduced overall function and strength.
- Like a lot of people post-surgery, she was unsure of how much to push things so needed reassurance, which is very common especially if pain involved.
Therapy
The session would start with a heat pack for ten mins. This was followed by continuous passive motion (CPM) on the Primus (for about 3 mins) focused on abduction, forward flexion and external rotation of the left upper quadrant. This was used as a warm up and stretching. After a number of sessions, they also progressed and did some PNF with the cable attachment to give different planes of movement.
The team put together a battery of tests for breast patients so they could standardise. This data was then used by the clinical team to monitor and manage each session and also shared with the patient.
The patient found the data so helpful, as you can clearly see that the right side is a lot stronger than the left (see below). It’s really important for the patient to continue with exercise at home so they were given theraband and a regime, then were tested on the BE Primus each appointment. Engaging the patient is really crucial and it also gives defined outcome measures.
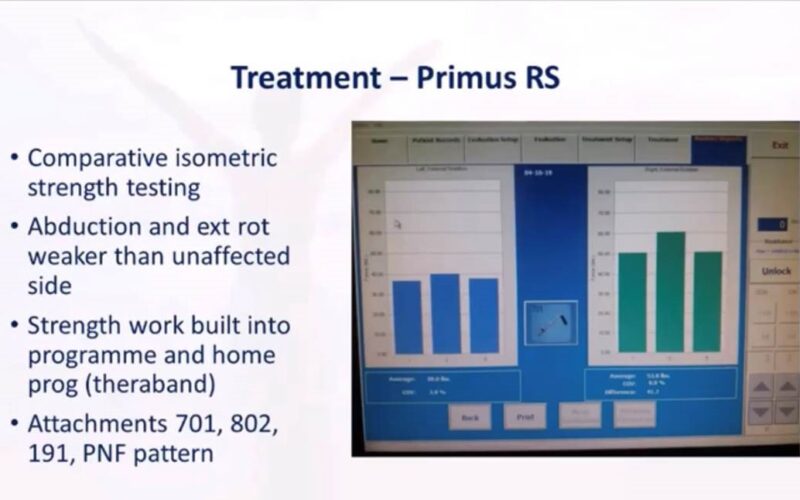
Graph showing before treatment
It’s really important to ask patients what is important to them. Patients love the visual aspect and seeing a graph go up, showing improvement. It improves confidence and self-efficacy that they can complete a task. When you can simulate an activity it gives them great confidence in replicating their exact ADL or return to work tasks. Patients love these aspects.
Rosie Dear

The only main thing to address was the scarring. This patient was one of the first people the team used LymphaTouch with. LymphaTouch is a targeted negative pressure system which allows the tissue to be manipulated in a controlled way. This can be done in continuous, pulse and mechanical vibration modes. There was initial discomfort, but each session it improved and the patient became more comfortable with the treatment.
For this type of patient, the LymphaTouch is used more as a localised way to release soft and scar tissue, in this case around the mastectomy scar, rather than for Lymphoedema.
Treatment would start at 80mmHg pressure and go up to 180mmHg as required. They didn’t use LymphaTouch during active radiotherapy as tissue is sensitive. Tissue would always be monitored to see if there was any adverse reaction. The main aim was to ‘mobilise tissue’ so sometimes they used emollient and sometimes not, depending what the reaction was. The patient would be set up in different positions to enhance the results.
During this two-year program, they have had no adverse reaction of using it with any breast cancer patients.

As she was one of the first people through, Ms A had 19 appointments over 8 months which is much more than the 3 or 4 appointments most patient get. LymphaTouch treatments were 10-20 minutes on average. Time is in such short supply, so the team is really happy with the results they have been able to achieve in this time. Ms A was given home exercises and advice on the best sleeping position to help lengthen tissue. Patients are always given a self-management program so that they can progress at home. This is even more important due to the pandemic. Ms was able to return to work and all hobbies. Ms A still had some tightness and cording but nothing that had any impact on her performing tasks. One of the main goals for the OT team is to get patients back to ADLs and return to work activities. These tools play a really important role in achieving this.

Significant clinical improvements in several areas.

Data slide showing improvements on primus over 4 month period. Right and left have become more similar.
Service developments
- 2 years since conception. They get 3-4 referrals per month now and seeing them through lockdown.
- No negative feedback from the service.
- Radiographers are referring more and more. They are sometimes unable to reach the position required for radiotherapy. This service has helped all referred patients achieve the required positions with this, normally within in 1-2 sessions who have then been referred back to radiotherapy.
- OT is now being put in to the breast cancer therapy pathway.
- Going to use the donations to create a more like spar-like feel and less clinical.
Thank you to Rosie and all of the UHL team for putting this case study and presentation together. Thank you to Ms A for volunteering her information also.
Watch the full webinar below:



