
Overuse or repetitive trauma injuries represent approximately 50% of all sport-related injuries. It is speculated that more than half of these injuries may be preventable with simple approaches. [1]
– NATA (National Athletic Trainers’ Association),
Position Statement on Prevention of Pediatric Overuse Injuries
50% may be a low estimate. What are you doing to reduce your athletes’ chances of injury?
As a Physiotherapist, Sports Therapist, Chiropractor, Osteopath, or Massage Therapist you rely on a variety of manual therapy tools to help address daily sports-related overuse and repetitive trauma injuries, and post-surgical challenges.
While we all have our favourite tools, whether it’s our go-to IASTM instrument or our hands, we’ve learned that no single device or technique does it all. A variety of techniques are needed to achieve positive outcomes like getting our athletes back on the field, performing at elite levels, or helping prevent injuries in the first place.

So it’s important to continue to learn about new innovations that can help us achieve results… and have a variety of COMPLEMENTARY modalities in our toolbox.
POSITIVE PRESSURE THERAPY
Positive pressure therapies include any protocol where you’re creating downward pressure into the tissues.
Positive pressure therapies include:
- Soft Tissue Massage
IASTM Instruments and Techniques
Trigger Point/Acupressure
Foam Rolling or Other Forms of Self-Myofascial Release (SMR)
High-Speed Vibration
ART/PRT/SPRT
Percussive Therapeutic Massage
Almost all manual therapy techniques create positive pressure downward into the tissue. These techniques, like massage, are research-proven to help reduce your patient’s pain or fatigue.
2018 Study: Systematic Review with Meta-Analysis on An Evidence- Based Approach for Choosing Post-Exercise Recovery Techniques to Reduce Markers of Muscle Damage, Soreness, Fatigue, and Inflammation…Dupuy et al., [2]
Key Results: Maximising the performance capacity of an athlete is not only a matter of training. It also depends on an optimal balance between training and recovery in order to prevent maladaptation to accumulated psychological and physiological stresses induced by the training load (Meeusen et al., 2013; Soligard et al., 2016) [3,4]. Massage seems to be one of the most effective methods for reducing DOMS (delayed onset muscle soreness) and perceived fatigue.
But once again, whether you rely on your hands or your favourite therapeutic device to facilitate your manual therapy, all of the approaches create positive pressure to increase function and mitigate restrictions in the tissue.

This is why myofascial decompression or negative pressure therapy is the perfect COMPLEMENT to your current treatment protocols and a crucial modality to understand.
NEGATIVE PRESSURE THERAPY
Negative pressure therapy is another way you can address musculoskeletal and fascial challenges and maladaptations in your patients.
CUPPING THERAPY
One example of negative pressure therapy is Myofascial Decompression (MFD) or Dry Cupping. This method has been around for thousands of years. MFD uses a cupping device to create a suction and negative pressure.
MFD mechanically increases blood circulation while physiologically activating the immune system to stimulate the mechanosensitive fibers and reduce your patient’s pain. There is initial scientific evidence that dry cupping is able to reduce musculoskeletal pain.[5] It has also been proven to be an effective modality for improving health and function.
LYMPHATOUCH TAKES MFD TO A NEW LEVEL

The innovative LymphaTouch vibrational active negative-pressure treatment device combines the benefits of myofascial decompression with the added benefits of vibration.
This creates a comfortable, effective solution that helps improve your outcomes and helps your patients reach their goals.
HOW DOES LYMPHATOUCH COMPARE TO CUPPING?
With our increased awareness of the fascial system, it’s important to note that new lymph vessels cannot grow through scar tissue or fibrosed tissues. Cupping, which has become very popular, only offers a static negative pressure against the skin in a very local area. The use of a negative pressure device like the LymphaTouch allows gliding along the skin from ‘foot to face’, which can facilitate and stimulate the natural peristaltic contractions of the two to three layers of muscles located along the lymphatic pathways, also called lymphangions (Mislin, 1961).
– Dr. Jeffrey Tucker, DC
President of the ACA Rehab Council
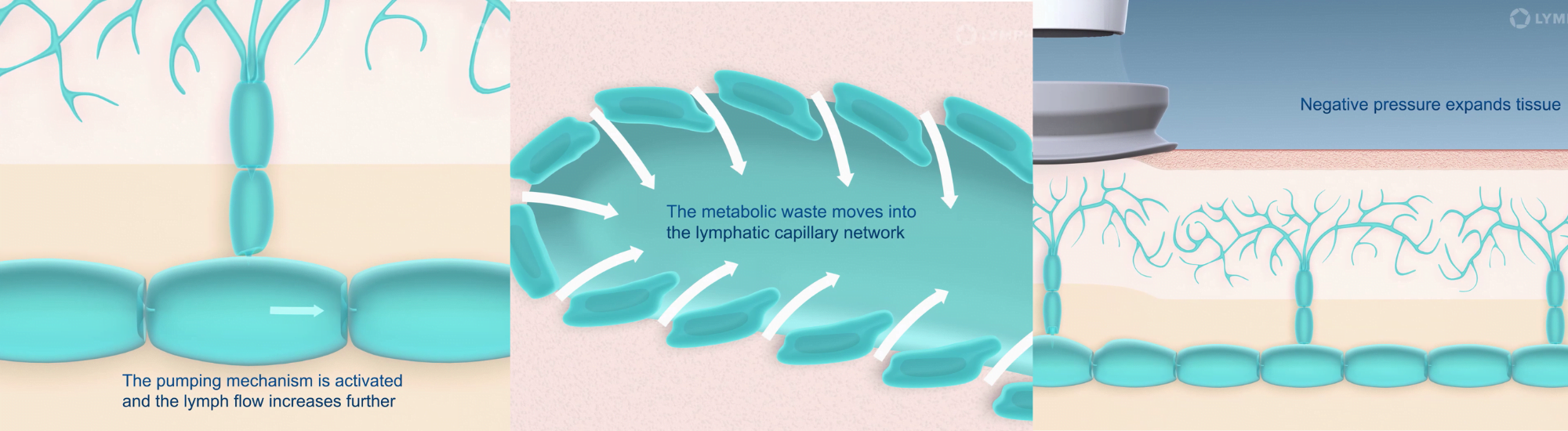
LymphaTouch generates active negative pressure that helps improve lymphatic circulation in the treated area. It also has a mechanical high-frequency vibration feature.
WHEN CAN LYMPHATOUCH BE USED?
The LymphaTouch device can be applied to several treatment areas to help manage a variety of conditions, including:
- Pain management
Pre and postoperative swelling and scarring
Muscle maintenance
Active recovery
Fascial tightness
Compromised joint function
Lymphoedema
Improve your patients’ rehabilitation using the LymphaTouch device. The combination of negative pressure and mechanical high-frequency vibration enhances lymphatic circulation making your treatment faster and more efficient.
CONTROL THE LEVELS OF DECOMPRESSION
The LymphaTouch allows you to control the levels of decompression on your patients. This makes a big difference!
When you use traditional cupping, you can’t determine the amount of negative pressure inside the cup. It’s just not possible. This means cupping can easily lead to bruising and other challenges, especially in hypersensitive tissue.
But the LymphaTouch provides graded negative pressure treatment which gives you the opportunity to control the decompression of the tissue (Donahue, 2019). This adds to the benefits of the localised vibration to provide additional overall benefits to the treatment.
Paula Donahue, PT, DPT, explains:
An additional feature when using graded negative pressure is the ability for the therapist to document the quantified amount of tissue pull tolerated by the patient from 20-250mmHg. For example, a patient with chronic knee pain following a total knee replacement may initially only tolerate graded negative pressure tissue mobilisation of 50-60mmHg, but following a few minutes of treatment, that same tissue location may begin to tolerate 70mmHg and then progress to a pull of 150mmHg within 1 to 2 visits. This provides objective documentation of the tolerable changes occurring for the patient in the mobilisation of the tissue. Simultaneously, the patients oftentimes experience increased joint movement and reduced pain or tenderness to touch.
Using graded pressure allows the clinician to reduce the intensity of the pull on the tissue to stay within the patient’s tolerance to treatment. The device also has the feature of adjusting the working and resting phase from 0.5 to 5 seconds. During the resting phase, the therapist can continuously adjust the exact location of treatment further ensuring no trauma to the tissue. Graded negative pressure application is easy to use and intuitive using touchscreen features to adjust compression and length of work and rest phases. Four treatment head sizes allow for convenient fit from smaller body regions (i.e. hands, feet, and angulations of face) to larger body sizes of the back and thigh. The key is to use the largest treatment head size possible while still obtaining full skin contact for adequate suction.[6]
WANT TO LEARN MORE ABOUT NEGATIVE PRESSURE THERAPY?
Stay tuned for the next article in this series on negative pressure therapy and LymphaTouch®.
References
1. Tamara C. Valovich McLeod, Laura C. Decoster, Keith J. Loud, Lyle J. Micheli, J. Terry Parker, Michelle A. Sandrey, and Christopher White (2011) National Athletic Trainers’ Association Position Statement: Prevention of Pediatric Overuse Injuries. Journal of Athletic Training: Mar/Apr 2011, Vol. 46, No. 2, pp. 206-220.
2. Dupuy O, Douzi W, Theurot D, Bosquet L, Dugué B. An Evidence-Based Approach for Choosing Post-exercise Recovery Techniques to Reduce Markers of Muscle Damage, Soreness, Fatigue, and Inflammation: A Systematic Review With Meta-Analysis. Front Physiol. 2018;9:403. Published 2018 Apr 26. doi:10.3389/fphys.2018.00403
3. Meeusen R., Duclos M., Foster C., Fry A., Gleeson M., Nieman D., et al. . (2013). Prevention, diagnosis, and treatment of the overtraining syndrome: joint consensus statement of the European College of Sport Science and the American College of Sports Medicine. Med. Sci. Sports Exerc. 45, 186–205. 10.1249/MSS.0b013e318279a10a
4. Soligard T., Schwellnus M., Alonso J. M., Bahr R., Clarsen B., Dijkstra H. P., et al. . (2016). How much is too much? (Part 1) International Olympic Committee consensus statement on load in sport and risk of injury. Br. J. Sports Med. 50, 1030–1041. 10.1136/bjsports-2016-096581
5. Rozenfeld E, Kalichman L. New is the well-forgotten old: The use of dry cupping in musculoskeletal medicine. J Bodyw Mov Ther. 2016;20:173-178.
6. Paula Donahue, PT, DPT, MBA, CLT-LANA Manual Strategies: Optimizing Patient Outcomes in the Clinic. Mar 25, 2019
ABOUT AUTHOR: DR. JOHN PECORA, DC
Dr. John Pecora is a Sports Chiropractic Specialist and Dean’s List graduate of Southern California University of Health Sciences and has been in private practice since 2004.
Dr. Pecora has worked with and treated athletes from the NFL, NHL, MLB, NBA, PGA, ASP/WSL, AVP, X Games, Olympics, as well as Collegiate athletes…and specializes in manual therapy (SPRT/ART),IASTM (Graston/HawkGrips), Kinesiology Taping (Kinesio, RockTape, FMT, TheraBand), joint mobilization and manipulation, numerous TherEx protocols, as well as numerous modalities including laser, PEMF, HSVT (High- Speed Vibration Therapy), PTM (Percussive Therapeutic Massage), MFD (Myofascial Decompression), Dry Needling, EPAT…and has his PES (Performance Exercise Specialist) from NASM (National Academy of Sports Medicine).
